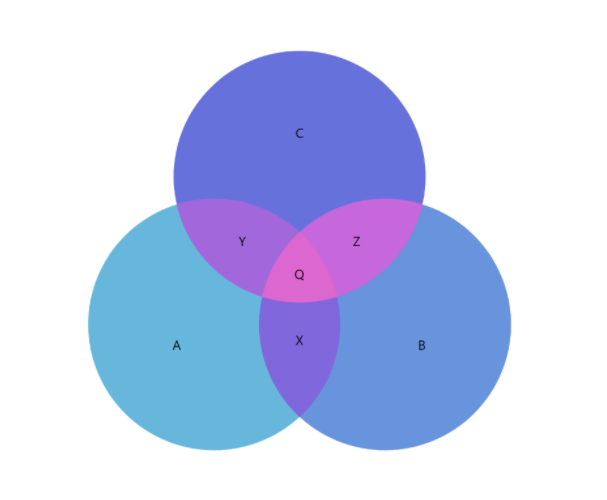
Over the years, I seem to have had this question come up on a fairly consistent basis and the answer is actually relatively straightforward. Let’s take as an example, an arbitrary portion of the scalp which is innervated by 3 different nerves. What that means is that three different nerves each supply sensation to the same piece of scalp skin. When someone touches that area, sensation is mediated to some degree by each of those nerves, all of which likely branch to some degree within that particular area. In other words, the areas of sensation mediated by each of those nerves likely overlap, much like area ‘Q’ in the Venn diagram below.
Now let’s assume that one of those nerves is injured. It is likely that the person in question now has some degree of discomfort in that area. If a procedure is performed in which that injured nerve is transected (i.e. cut) and implanted deep within the local muscle, hopefully with time, the painful sensations mediated by that nerve also diminish. However, s/he still has two nerves which innervate that portion of skin. When that same person touches that area of skin, s/he will feel it almost the same as before the operation. This person has no idea which nerve is mediating that perception of feeling, but for all practical purposes, it doesn’t matter. Hopefully, this explanation clears up some confusion. This phenomenon of overlapping nerve territories also explains why patients tolerate the transection/burial of some nerves better than others. It is not the only reason to consider when deciding whether or not a nerve can be transected and buried in the local muscle, but it is an important one.